儿童远视的特征
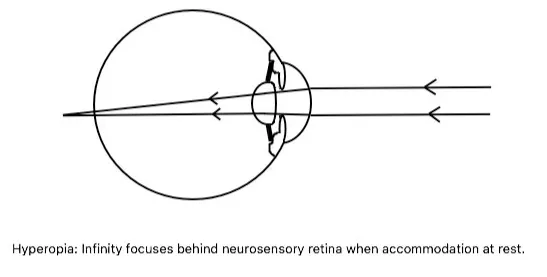
儿童时期最常见的屈光不正是远视[1]。远视这个术语指的是眼睛的屈光状态,当调节处于静止状态时,来自无限远处的平行光线(通过眼部屈光介质折射后)被聚焦在视网膜神经感觉层后面。
在出生时,人类主要是远视眼,并且随着年龄的增长,远视眼会变为正视甚至近视[2-3]。阳性家族史对下一代远视的发展起着至关重要的作用[4]。如果确诊后不进行治疗,可能会出现弱视和斜视等后遗症[5-6]。
远视的分类(按病因)
轴性远视(最常见的-单纯性远视):是由于眼球前后轴向过短所致。遗传倾向起着重要作用。视网膜水肿可引起远视性漂移。轴向长度每减少1毫米,约导致3D远视屈光度[7]。
曲率性远视:这是由于角膜或晶状体变平或两者都变平所致。曲率半径每增加1 mm,远视屈光度约增加6D。
指数性远视:这是由于晶状体的折射率改变所致,这种情况发生在老年人或糖尿病患者身上。
位置性远视或晶状体缺失(无晶体眼)或眼部病理情况:这种情况的发生是由于晶状体(先天性或后天)或人工晶状体错位或缺失,原因是屈光介质中形成了无晶状体区域。外伤后或手术后的无晶状体眼是远视的常见原因。
少数眼部病变,如小眼球、无虹膜,可能导致远视。迄今为止,尚未确定一致的致病因素。虽然是偶发性的,但很少有遗传因素与远视有关。除了遗传和环境因素外,很少有后天条件造成远视的原因,特别是在老年人身上[8]。
学龄前不同阶段远视患病情况
近期发表于 Ophthalmology 上的一篇文献,调查了学龄前儿童远视的患病率。此研究由3个不同国家的4个研究组成儿童眼病研究联盟,共包括17214名儿童的眼科检查数据[9]。结果显示6~72月龄儿童视力较差眼远视(>200度)患病率为20.5%,中度/高度远视(≥400度)的患病率为3.2%,占所有远视的15.6%,中高度远视并不罕见。
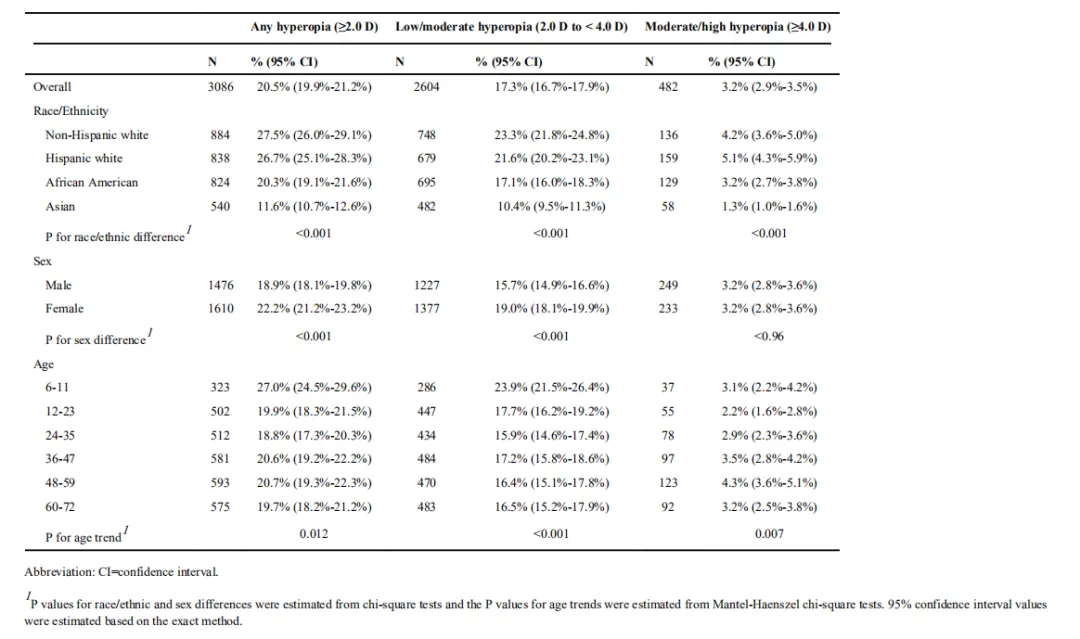
中低度远视在6-11月龄儿童中患病率最高,在24月龄后基本稳定;而中高度远视不随年龄而减少,除12-23月龄患病率略低,其他更高年龄段与6-11月龄相近或更高。表1列出按种族或族裔,性别和年龄分组的6~72月龄儿童较差眼的低中度远视(200~400 度)和中高度(≥400 度)远视患病率。
表1:按种族或民族、性别和年龄划分的儿童较差眼远视严重程度的患病率
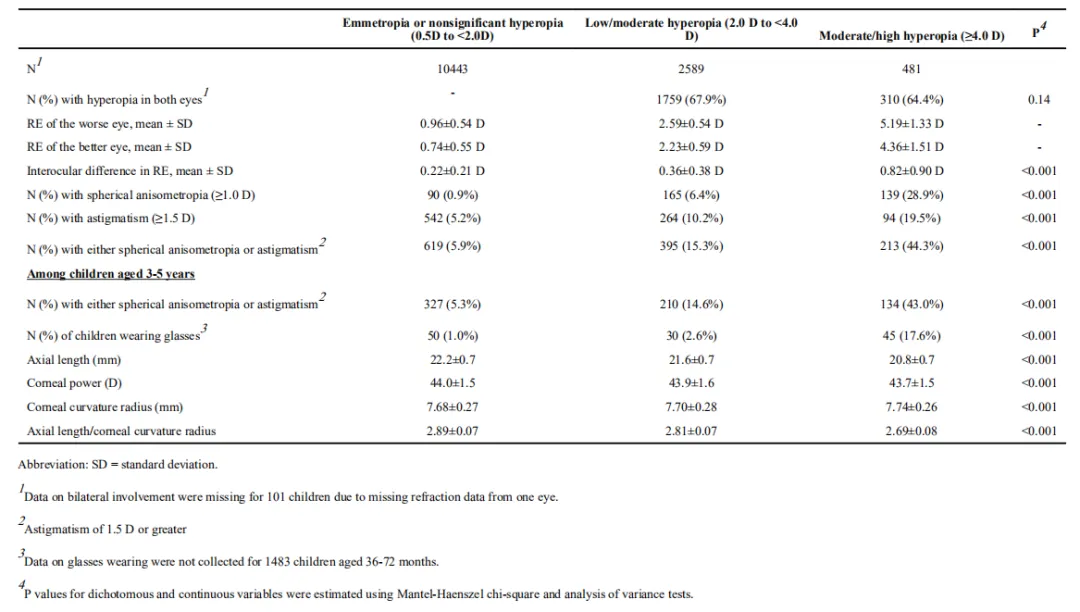
此外,在中高度远视儿童中,有较高比例存在双眼屈光参差。远视度数相差达100度或散光差达150度的比例为44.3%。屈光参差增加了斜视或弱视的风险。表2显示36~72月龄戴镜儿童较差眼不同类型远视的特征。
表2:儿童较差眼不同类型远视的特征
远视的危害
远视可能会导致视力下降,影响生活质量,轻度时可能无症状。人眼会自发通过调节增加晶状体屈光力来克服远视,额外的调节力可能会导致眼睛疲劳、头痛、间歇性模糊、身体平衡差、难以近距离阅读及认知能力、阅读能力、注意力下降等问题[10-17]。此外,学龄前儿童的调节不如成人准确,调节滞后会随着需求的增加而增加,变得更加多变[18]。
严重的可能会导致弱视。中高度远视是儿童发生弱视的重要原因之一[19],弱视会影响儿童视觉功能的发育与建立,在6岁以前儿童的视觉功能是一段较为敏感的时期,即视觉发育可塑性关键期[20-21]。相关的统计数据显示,有2%~4%的成人其视力下降是由于儿童时期的弱视和屈光不正发展而来的[22]。早期发现和纠正屈光不正,可以降低弱视发生率,使大部分弱视得到治愈同[23] 。
参考文献
[1]Castagno VD, Fassa AG, Vilela MA, Meucci RD, Resende DP. Moderate hyperopia prevalence and associated factors among elementary school students. Cien Saude Colet. 2015 May;20(5):1449-58. [PubMed]
[2]Semeraro F, Forbice E, Nascimbeni G, Cillino S, Bonfiglio VME, Filippelli ME, Bartollino S, Costagliola C. Ocular Refraction at Birth and Its Development During the First Year of Life in a Large Cohort of Babies in a Single Center in Northern Italy. Front Pediatr. 2019;7:539. [PMC free article] [PubMed]
[3]Yahya AN, Sharanjeet-Kaur S, Akhir SM. Distribution of Refractive Errors among Healthy Infants and Young Children between the Age of 6 to 36 Months in Kuala Lumpur, Malaysia-A Pilot Study. Int J Environ Res Public Health. 2019 Nov 27;16(23) [PMC free article] [PubMed]
[4]Tarczy-Hornoch K. The epidemiology of early childhood hyperopia. Optom Vis Sci. 2007 Feb;84(2):115-23. [PubMed]
[5]Lin PW, Chang HW, Lai IC, Teng MC. Visual outcomes after spectacles treatment in children with bilateral high refractive amblyopia. Clin Exp Optom. 2016 Nov;99(6):550-554. [PubMed]
[6]Laiginhas R, Figueiredo L, Rothwell R, Geraldes R, Chibante J, Ferreira CC. Long-term refractive outcomes in children with early diagnosis of moderate to high hyperopia. Strabismus. 2020 Apr 22;:1-6. [PubMed]
[7]Strang NC, Schmid KL, Carney LG. Hyperopia is predominantly axial in nature. Curr Eye Res. 1998 Apr;17(4):380-3. [PubMed]
[8]Harb EN, Wildsoet CF. Origins of Refractive Errors: Environmental and Genetic Factors. Annu Rev Vis Sci. 2019 Sep 15;5:47-72. [PubMed]
[9]Jiang Xuejuan,Tarczy-Hornoch Kristina,Stram Douglas et al. Prevalence, Characteristics, and Risk Factors of Moderate or High Hyperopia among Multiethnic Children 6 to 72 Months of Age: A Pooled Analysis of Individual Participant Data.[J] .Ophthalmology, 2019, 126: 989-999.
[10]Arnold RW. Pseudo-false positive eye/vision photoscreening due to accommodative insufficiency. A serendipitous benefit for poor readers? Binocul Vis Strabismus Q. 2004; 19:75–80. [PubMed: 15180592]
[11]Simons HD, Gassler PA. Vision anomalies and reading skill: a meta-analysis of the literature. Am J Optom Physiol Opt. 1988; 65:893–904. [PubMed: 3252737]
[12]Stewart-Brown S, Haslum MN, Butler N. Educational attainment of 10-year-old children with treated and untreated visual defects. Dev Med Child Neurol. 1985; 27:504–13. [PubMed: 4029521]
[13]Grisham JD, Simons HD. Refractive error and the reading process: a literature analysis. J Am Optom Assoc. 1986; 57:44–55. [PubMed: 3512675]
[14]Kulp MT, Ciner E, Maguire M, et al. Uncorrected hyperopia and preschool early literacy: results of the Vision in Preschoolers -Hyperopia in Preschoolers (VIP-HIP) Study. Ophthalmology 2016;123(4):681–9. [PubMed: 26826748]
[15]Moon Byeong-Yeon,Choi Jae Hyeok,Yu Dong-Sik et al. Effect of induced hyperopia on fall risk and Fourier transformation of postural sway.[J] ., 2019, 7: e8329.
[16]van Rijn Laurentius J,Krijnen Jacqueline S M,Nefkens-Molster A Eline et al. Spectacles may improve reading speed in children with hyperopia.[J] .Optom Vis Sci, 2014, 91: 397-403.
[17]Marjean Taylor Kulp, OD, MS, et al.Uncorrected Hyperopia and Preschool Early Literacy: Results of the Vision In Preschoolers - Hyperopia In Preschoolers (VIP-HIP) Study.Ophthalmology. 2016 April ; 123(4): 681–689. doi:10.1016/j.ophtha.2015.11.023.
[18]Anderson HA, Glasser A, Stuebing KK, Manny RE. Minus lens stimulated accommodative lag as a function of age. Optom Vis Sci. 2009; 86:685–94. [PubMed: 19417707]
[19]Atkinson J, Braddick O, Robier B, Anker S, Ehrlich D, King J, et al. Two infant vision screening programmes: prediction and prevention of strabismus and amblyopia from photo- and videorefractive screening. Eye. 1996; 10: 189–198.
[20]刘满军.对学龄前儿童屈光及视力发育情况的调查分析,当代医药论丛[J].2019年第17卷第16期.
[21]Goggin Michael, Zamora-Alejo Katherine, Esterman Adrian, et al. Adjustment of anterior corneal astigmatism values to incorporate the likely effect of posterior corneal curvature for toric intraocular lens calculation.. Journal of Refractive Surgery, 2015, 31(2):98-102.
[22]周薇薇,韩冰,等.深圳市龙岗区初中生视力发育及屈光状态的流行病学调查[J].中国妇幼保健,2017年17期.
[23]卞巧月,陈科锦,等.1~7岁儿童不同阶段屈光发育调查分析[J].中国药物